Values Clarification
Challenging Patient Encounters Digital Module
Family Planning and Abortion
Think about an experience in which you felt frustrated with or angry at a patient…
How did it make you feel?
What made you feel that way?
Common scenarios mentioned by other medical and nursing students include:
- Patients who were very frustrated and yelled at them
- Patients who didn't tell them the truth about their health behaviors
- Patients who smoke or use other substances that were causing harm to their health
Empathy
Once you can recognize your feelings of frustration, you can work on these feelings so they don’t interfere in the patient-clinician relationship.
Think about the patient interaction that made you feel upset or angry.
Now, shift focus from your own feelings.
Put yourself in the patient’s shoes.
Why do you think your patient did or was doing whatever it was that upset you?
Are there aspects of the patient's life (current or past situations, experiences, beliefs, feelings, values, environment) that may explain or help you understand their behaviors?
Compassion
If it’s hard to put yourself in the patient’s shoes, try simply imagining that the patient is having a hard time.
Does this help you feel compassion toward him or her?
Now think about how you reacted to the situation with the patient.
Do you think it affected how you cared for the patient?
Do you think the patient noticed that you were frustrated?
Is there anything you could have done to be a better provider?
We know building rapport with patients can greatly improve outcomes.
Studies show that patients who perceive their providers as kind and nonjudgmental are more likely to:
- be satisfied
- follow treatment plans
- return for follow-up
- take better care of themselves overall
But a good “poker face” isn't enough.
A lot of us think patients don’t notice when we’re frustrated with them, but evidence strongly suggests otherwise.
It’s sometimes hard to imagine we could expose our negative feelings to patients, but becomes more believable when we remember seeing it.
Think of a time when you saw a clinician interacting with a patient that exposed their frustration or anger.
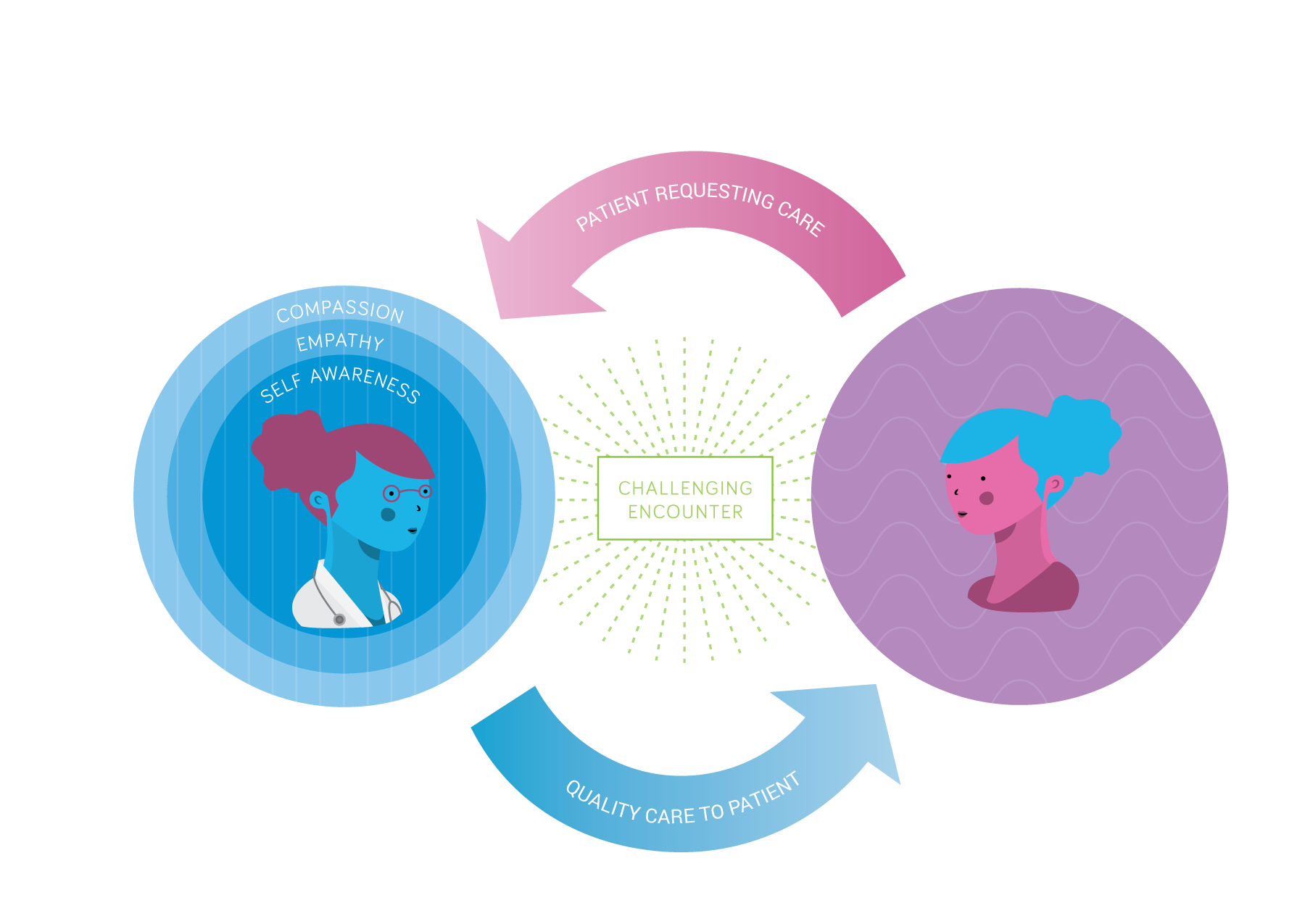
By showing empathy and compassion, we can discard the “poker face” and replace it with real concern and understanding that patients can see, hear, and feel.
Building self-awareness, empathy, and compassion can also reduce your frustration in challenging situations, lessen feelings of personal failure, and help you accept your limitations as a provider.
Unintended pregnancy is extremely common.
In the United States, more than half of all women will experience an unintended pregnancy by the age of 45.
Half of all women who experience an unintended pregnancy will have an abortion.
Abortion is extremely common.
In the United States, 21% of all pregnancies (excluding miscarriages) end in abortion.
Nearly 1 in 3 women have had an abortion by the age of 45.
Source: Guttmacher Institute
Let's take an inventory.
I am generally comfortable with a patient choosing to parent in the following circumstances:
How do your feelings change if the patient is 16?
How do your feelings change if the pregnancy is further along (e.g., toward the end of the second trimester, at 22 weeks gestation)?
I am generally comfortable with a patient choosing adoption in the following circumstances:
How do your feelings change if the patient is 16?
How do your feelings change if the pregnancy is further along (e.g., toward the end of the second trimester, at 22 weeks gestation)?
I am generally comfortable with a patient choosing to have an abortion in the following circumstances:
How do your feelings change if the patient is 16?
How do your feelings change if the pregnancy is further along (e.g., toward the end of the second trimester, at 22 weeks gestation)?
Your patient is a 23 year old woman. She's eight weeks pregnant. This is her first pregnancy.
Do you feel you can provide supportive, nonjudgmental, comprehensive options counseling (parenting, making an adoption plan, having an abortion)?
If she chooses abortion, would you feel comfortable making a referral?
Take a moment to notice and reflect on any feelings you may have about this patient.
Would your feelings change if the patient is pregnant because of a contraceptive failure?
You are counseling a woman who desires an abortion.
After you explain what to expect during the abortion, you move on to discuss contraception.
She tells you that she isn’t planning to use contraception.
Take a moment to reflect on any feelings you may have about this patient.
What are some of the reasons your sexuality active patients don't use contraception?
A sexually active woman who does not use contraception has an 85% chance of getting pregnant within a year.
There are numerous reasons patients don't use contraception.
- Fatalistic outlook about pregnancy (e.g., “When it's your time to get pregnant, you will.”)
- Belief that they're infertile or can't get pregnant
- Dislike or fear of side effects
- Doubt about the effectiveness of contraception
- Lack of contraceptive knowledge
Sources
Many patients experience institutional, social, and cultural barriers when trying to access contraception.
- History of contraceptive coercion or manipulation within minority communities
- Stigma surrounding long-acting, reversible contraception (LARC)
- Health disparities
- Health care disparities
- Difficulty accessing care
- Diminished public funding for contraception
- Complex reimbursement systems under the Affordable Care Act
- Negative encounters with clinicians
Take a moment to reflect on how these barriers can influence a woman's choice to use—or not use—contraception.
How do these barriers affect your feelings or attitudes toward your patients?
Your patient is 23 weeks pregnant. She's decided to have an abortion.
Please take a moment to notice and reflect on any feelings you may have about this patient.
It's common to feel judgmental or angry with patients who “wait” until later in pregnancy to have an abortion.
Put yourself in the patient's shoes—what are some reasons a woman might present late?
Research shows that, on average, women report 2.2 reasons for presenting 16 weeks after their last menstrual period.
Reasons include:
- Didn't realize she was pregnant (71%)
- Difficulty making arrangements to have an abortion (48%)
- Afraid to tell parents or partner (33%)
- Needed time to make her decision (24%)
- Hoped relationship would change (8%)
- Pressure not to have abortion (8%)
- Something changed during the pregnancy (6%)
- Didn't know timing was important (6%)
- Didn't know she could have an abortion (5%)
- Fetal abnormality diagnosed late (2%)
Torres and Forrest, 1988
Patients who present in the second trimester face more logistical barriers than patients in the first trimester.
On average, patients in the second trimester cited three reasons that delayed their procedure.
Barriers include:
- Figuring out where to go
- Referral from other clinics
- Arranging transportation
- Difficulty getting state-funded insurance
Drey et al. 2006
As healthcare providers, it’s our duty to provide patient-centered care and separate our personal feelings from the care we provide.
It’s natural for us to feel judgmental or to react to patients’ behaviors that push our buttons, but it’s important for us to be aware of when we feel uncomfortable or judgmental and be prepared to handle it so that we can maintain a therapeutic relationship with the patient and provide patient-centered care.
Thank you!
We’d love to hear your feedback.
Please send all comments and suggestions to info@innovating-education.org