Search Results for: aspiration
Sort
Filter by Topic
Filter by Type
Courses
Resources
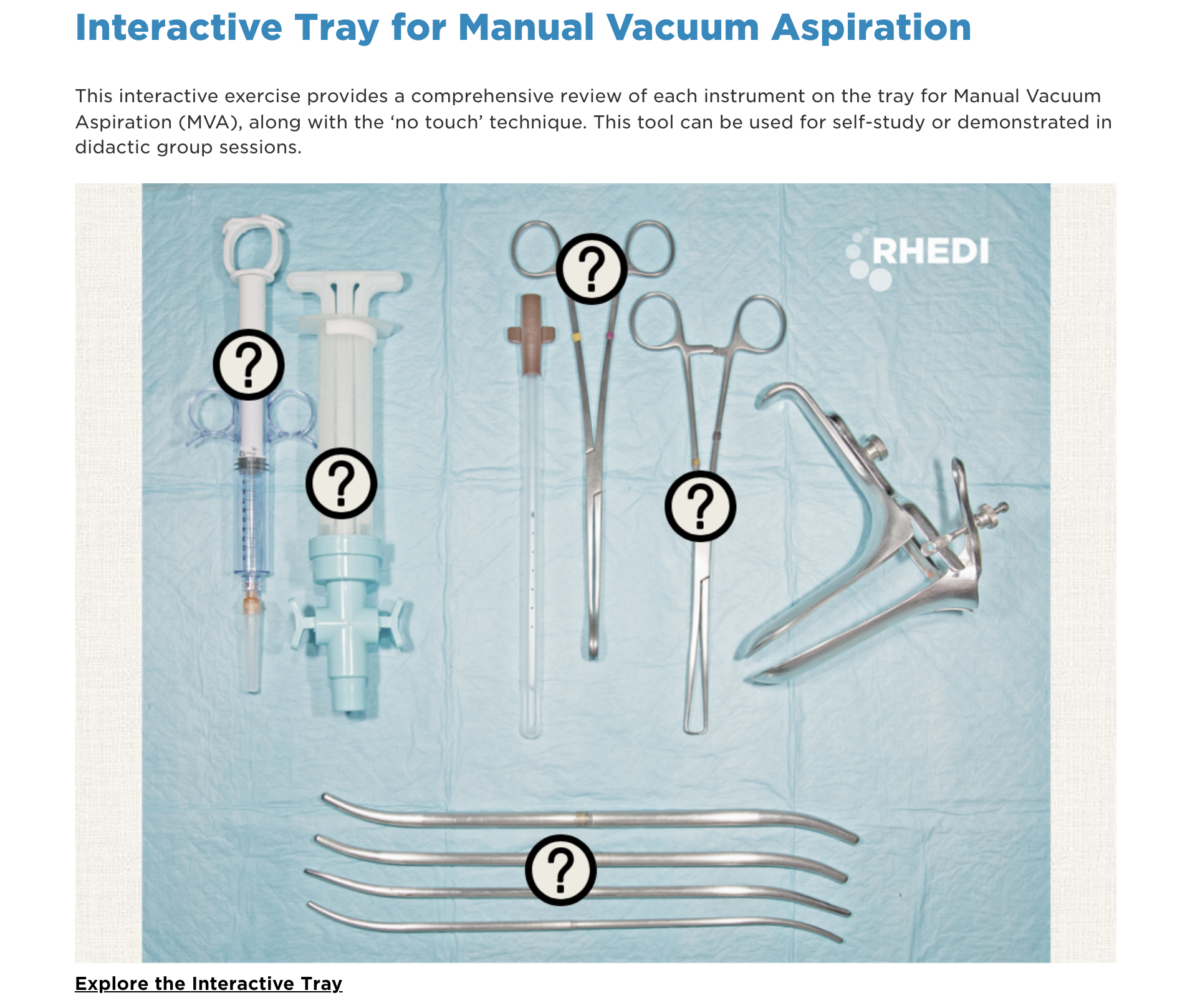
Interactive Tray for Manual Vacuum Aspiration
Uterine Aspiration Abortion – Ryan Curriculum
Uterine Aspiration Procedure
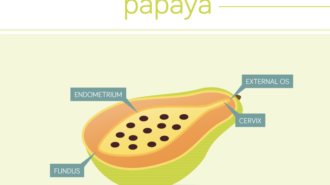
RHEDI Virtual Papaya Workshop
Uterine Aspiration Procedure for EPL
First Trimester Aspiration Abortion
Uterine Aspiration Procedure 1
Uterine Aspiration Procedure 2
Uterine Aspiration for Early Pregnancy Loss
Abortion Course Update!
We are excited to announce 5 new videos have been added to our Abortion Course! Visit the course page to see the update and all original content!
Medication Abortion – presented by: Lealah Pollock, MD, MS
Counseling for Pregnancy Ambivalence – presented by: Alissa Perucci, PhD, MPH
Contraception 101 – presented by: Michalle Ramirez-McLaughin, RN, MS, FNP-BC
Uterine Aspiration Abortion – presented by: Sanithia L. Williams, MD
Prescribing Emergency Contraception – presented by: Shokoufeh Dianat, DO
Visit the Abortion Course to view the original videos and the course update!
Counseling for EPL Management Options
This is How I Teach: Uterine Aspiration
First-trimester Aspiration Abortion Slide Set
EXPLAINED: Abortion Safety in the United States Lecture
EXPLAINED: Abortion Safety in the United States
Teaching Pain Management for Uterine Aspiration

Abortion Safety in the United States
Abortion Safety in the United States Lecture
Changing the Conversation: Shared Decision-Making in Reproductive Health

Pain with Uterine Aspiration Abortion Slide Set
Pain with Uterine Aspiration Abortion
First-Trimester Aspiration Abortion
EXPLAINED: Who Can Safely Provide Abortion? Lecture
EXPLAINED: Who Can Safely Provide Abortion?
Animated Uterine Aspiration Simulation Workshop
EXPLAINED: Targeted Regulation of Abortion Providers Lecture
EXPLAINED: Targeted Regulation of Abortion Providers
Targeted Regulation of Abortion Providers (TRAP Laws) Lecture
Targeted Regulation of Abortion Providers (TRAP Laws)
The Papaya Workshop
Snap Shots
Success stories from physicians who have incorporated abortion services in a way that works for them.
Private Practice
Academic Practice
HMO
Moonlighting
Private Practice: Jill
Jill is a generalist ob-gyn in multi-specialty group practice who has incorporated abortion provision as a component of her a busy practice. While the total number of abortions she performs each month varies, she has made it a priority to squeeze in patients who need abortion services and provide them with excellent care. Most of the patients Jill sees for abortions are already part of her practice, but she also accepts referrals from high-risk obstetricians for patients with chromosomal abnormalities or from new patients whose first visit is for an abortion but often become regular patients. Because she already has relationships with many of her abortion patients, Jill is able to tailor the counseling to their specific situation which uses her time more efficiently while also providing each woman what she needs.Much like patients with miscarriages, women seeking pregnancy terminations need to receive care as soon as possible. To meet this need, Jill can fit in a consultation for a first-trimester procedure in within a few days. At that first appointment, she will provide counseling, pregnancy dating, and help the patient decide whether to have a surgical or medication abortion. If the latter, the patient can start the process the same day by taking Mifipristone in the office and scheduling appropriate follow-up care. For surgical abortions, Jill will bring the patient back into the office for a simple MUA procedure or will schedule the patient in the OR if they are at a later gestation or require more anesthesia. In-office MUA procedures are quick and simple; by scheduling them at the end of the morning or afternoon scheduling block, they can have plenty of time to recover without inhibiting the flow of patients being seen for routine care.
Private Practice: Wayne
Wayne works in a full service general ob-gyn practice in New England where he has integrated in-office abortion procedures up to 13 weeks for many years. Requests for abortions are treated and scheduled like any other appointment. Patients are counseled about their abortion options over the phone and are scheduled for a visit either with a nurse practitioner for a medication abortion or with Wayne for a surgical abortion. For aspirations, patients are scheduled for a one-hour appointment during which the patient will discuss the procedure and receive counseling from Wayne, she will then have the procedure and recover in an exam room. Wayne can often see another patient during the hour while the patient is prepared for the procedure by his staff.Wayne performs procedures on any patient requesting an abortion including referrals and patients never before seen in his office. He has found that many patients who come to him initially for an abortion will continue to utilize his practice for all their ob-gyn needs. He considers abortion provision to be a great “practice builder” because women who receive excellent, non-judgmental, compassionate care for an abortion become patients for life. Patients learn that they can access abortion in Wayne’s practice through word of mouth, online through the practice website or abortion.com, or by referral.
Private Practice: Stephanie
Stephanie is a generalist in a large multi-specialty group practice in the North East. When she started with this practice after residency, the group had an established pattern of referring out all abortion services. Stephanie developed a system to care for her own patients and accept referrals from women in need of second-trimester terminations within their group system. Typically, when Stephanie receives a referral from one of her partners, she finds a slot in her schedule for a pre-op visit within a few days and an OR slot the day after. Sometimes that means rescheduling a few other patients and doing the pre-op visit at lunch time. Because of a long tradition of terminating pregnancy in the hospital where Stephanie works, she hasn’t had any problems finding OR staff to assist her with these cases; however, she has had some trouble getting ultrasound techs from the Radiology department who are willing to participate.In addition, Stephanie works as part of a pregnancy loss team that performs MUA in the clinic setting for women with missed or incomplete abortions. This clinic is set up to use IV conscious sedation and has affiliated nurses who can care for the women with that level of anesthesia. Up to now, Stephanie has been unable to persuade the other team members to schedule first-trimester elective abortion patients in the pregnancy loss center as well. Instead, all first-trimester terminations are referred out to a free standing clinic. While her physician colleagues are supportive of providing elective terminations, there is resistance among the nursing staff.
HMO: Pratima
Pratima does abortions 2 days per week for patients at a large HMO that refers most patients seeking to terminate pregnancy to a freestanding clinic. Because freestanding clinics are not set up to see medically complicated patients, those patients are treated by Pratima in her hospital-based abortion service. This combination ensures that patients do not have their pregnancy options restricted by medical complications and that they can be seen promptly. Most of the patients that Pratima sees for pregnancy terminations do not come to her for their primary ob-gyn care. But, because of the integrated medical record within the health care system, she is able to access their full health history and provide enhanced continuity of care over a referral to a freestanding clinic.
Moonlighting: Andrea
Andrea works in a small group practice outside of Portland. At present, her partners have decided not to perform elective abortions within the practice. They do care for women with early pregnancy loss in the office setting with MUA. Andrea performs terminations at a free standing clinic 2 days per month. She and her partners refer patients seeking abortion to the same clinic. Over the next few years, she may try to include more elective procedures in her practice. In the meantime, her work at the abortion clinic helps her maintain her skills as an abortion provider.
Academic Practice: Jessica
Jessica is a generalist on faculty at the university where she did her residency training. She performs abortions both for her own patients and helps staff a second-trimester clinic for patients referred from the community and Perinatal center. On average, the weekly D&E clinic takes care of 4-5 patients with fetal anomalies in the OR. For her private patients, Jessica can perform MUA in the office or prescribe medication abortion on the same day. If the patient has medical complications or needs more anesthesia, she can be seen in the OR or at local planned parenthood with whom they maintain a strong cross-referral relationship.When Jessica joined the faculty, residents were already being trained to do abortions via a combination of hospital-based and free-standing clinics. But, the second-trimester service for patients with more medical complications was disorganized. By streamlining the scheduling process and organizing some education sessions for the staff, the clinic is now stable and running smoothly.
Abortion in the Primary Care Setting
Patient Decision Making about Abortion after the First Trimester
Global Maternal Newborn Health Conference
TEACH Simulation Training
Counseling for Miscarriage Management

The Importance of Family Planning Training in Zimbabwe: Part Two
Where are the Nurses in Abortion Care?

Notes From a Full Spectrum NurseMidwifery Student, Part I

Using Papayas to Promote Medical Student Interest in Obstetrics and Gynecology presentation
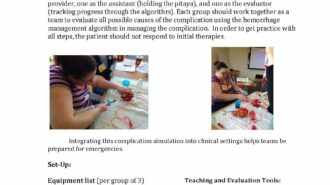
Managing Complications of Procedural Abortion Slide Set
Myths about Abortion Complications Slide Set
Notes From a Full Spectrum NurseMidwifery Student, Part II
Pages
Our Work
Abortion is a common experience for women around the world; yet it is often excluded from mainstream curricula. Our aim is to fill in these gaps by offering free and open source evidence-based family planning curricula.
Innovating Education cultivates clinicians who offer high-quality, patient-centered, comprehensive reproductive healthcare by generating, curating, and disseminating novel curricula, learning tools, and research for educators.
We encourage educators, trainers, and learners at all stages to incorporate our resources into their lectures, curriculum, and peer-to-peer activities.
All of our curated materials are given proper citation and author credentials. If you have curricula or tools you wish to share, contact info@innovating-education.org.
Courses
In fall of 2014, UCSF partnered with Coursera.org to create Abortion: Quality Care and Public Health Implications, the first online course about abortion. It had over 6,500 learners from 155 countries and featured over twenty faculty from various institutions and multiple disciplines. Our video lectures are now used in 80 ob-gyn residency training programs across the United States and Canada.
Managing Early Pregnancy Loss is an educational initiative incorporating video-based curriculum, clinical resources, and patient education materials to support an evidence-based and patient-centered approach to miscarriage management. Our curriculum provides a comprehensive review of diagnosis and treatment of early pregnancy loss (EPL) including didactic narratives, provider testimonials, and live video and animation demonstrating a step-by-step method for manual uterine aspiration (MUA). Since its launch, we have had over 4,000 users from more than 100 countries. Our video modules has been used by organizations such as WomanCare Global and Ipas for reproductive health care trainings around the world.
Professional Responsibility
Research shows that medical students exhibit a decline in empathy after they begin interacting with patients which poses a threat to their ability to provide patient-centered care. Patient-centered care challenges doctors to be empathetic, respectful, and compassionate, even during difficult patient interactions or when they have moral objections to the patient’s health behaviors. Teaching about abortion provides a learning opportunity for students to practice empathy and compassion in the face of patient behavior which they may not support.
Innovating Education works to ensure that all clinicians are prepared to fulfill their professional responsibility and provide patient-centered care regardless of their personal feelings about abortion and family planning. Through research and the development of workshops, interactive tools, and teaching materials, we prepare educators to teach empathy to health learners.
Where We’ve Been
2013
- Panel, Addressing Health Disparities through Family Planning Education, APGO-CREOG Annual Meeting
2014
- Invited Lecture, Online Resources for Teaching and Patient Care, Ryan Residency Training Program National Workshop
- Invited CME Webinar Lecture, UCSF Bixby Center for Global Reproductive Health, Train the Trainer: How to Facilitate a Values Clarification Session
- Panel, Sexual and Reproductive Health: Strategies to Broaden the Spectrum of Gynecology, Colombian Federation of Obstetrics and Gynecology (FECOLSOG)
- Invited Lecture, Importance of Education in Sexual and Reproductive Health in Gynecology Training, Colombian Federation of Obstetrics and Gynecology (FECOLSOG)
- Panel, Innovations in Sexual and Reproductive Health Education, North American Forum Society for Family Planning
- Invited Lecture, Digital Tools for Hands on Education Medical Students For Choice
2015
- Panel, Abortion and Family Planning Digital Curriculum, Training Access Working Group, Guttmacher Institute
- Panel, Integrating Opt-out Learners in Family Planning: Tools for Optimizing Learning and Clinical Care, National Abortion Federation
- Invited Lecture, Facilitating Client-centered, Values Clarification and Attitude Transformation, International Planned Parenthood Southeast Asia Regional Office
- Panel, Innovate Curricula for Teaching Family Planning and Safe Abortion, FIGO October 2015
- Invited Lecture, Innovating Education in Reproductive Health and Family Planning, Global Maternal Newborn Health October 2015
- Invited Lecture, Digital Education Tools for Ob/gyn Residents, Ryan Residency Training Program National Workshop, November 2015
2016
- Panel, Values Clarification About Family Planning as a Tool to Increase Professionalism, International Congress on Women’s Health and Unsafe Abortion, January 2016
- Invited Lecture, Papaya Workshop: Manual Vacuum Aspiration for Early Abortion and Miscarriage Management Care, American Medical Student Association, March 2016
- Panel, Abortion, Professional Responsibility, and Patient-Centered Care, American Medical Student Association, March 2016
- Panel, Reproductive Health within the Framework of Reproductive Justice, American Medical Student Association, March 2016